
Arthroscopic Synovectomy
Get Clear, Concise Answers to Your Top Questions About Arthroscopic Synovectomy
Q1. What is an arthroscopic synovectomy of the shoulder?
An arthroscopic synovectomy of the shoulder is a minimally invasive surgery used to remove the synovium, which is the thin lining that surrounds the shoulder joint. When this lining becomes chronically inflamed, swollen, or diseased, it can cause severe pain and joint damage. Using small incisions and a tiny camera called an arthroscope, your surgeon can clean out this damaged tissue to relieve pain and protect the joint.
Q2. What is the synovium, and what does it do?
The synovium is a thin membrane that lines the inside of your joints, including the shoulder. Its main job is to produce a small amount of fluid (synovial fluid) that lubricates the joint, allowing the bones to glide smoothly over each other. In a healthy joint, this lining is very thin. When it becomes diseased or inflamed, it thickens, produces excess fluid, and releases chemicals that cause pain and can gradually destroy the cartilage in your shoulder.
Q3. Why is an arthroscopic synovectomy performed?
This surgery is performed when the shoulder lining is chronically inflamed (synovitis) and does not improve with conservative treatments like medication, physical therapy, or cortisone injections. Common conditions that lead to a synovectomy include:
- Rheumatoid arthritis or other inflammatory autoimmune conditions.
- Chronic synovitis from osteoarthritis or joint overuse.
- Synovial chondromatosis (a rare condition where the lining grows nodules that turn into loose bodies).
- Pigmented villonodular synovitis (PVNS), a benign growth of the joint lining.
- Recurrent or chronic joint infections that require cleaning.
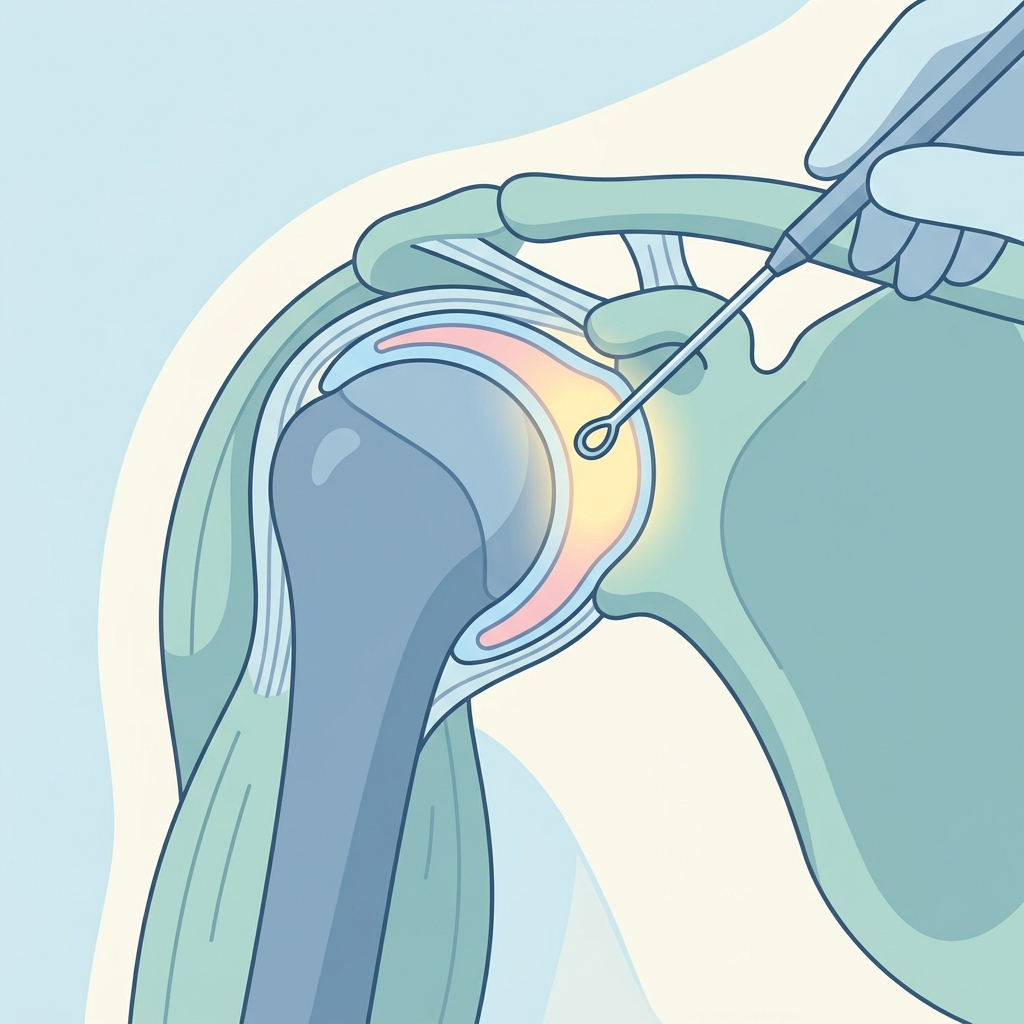
Q4. How is the surgery performed?
The procedure is done using shoulder arthroscopy, which is a keyhole surgery. Your surgeon will make a few tiny incisions (portals) around your shoulder. A small camera (arthroscope) is inserted through one incision to project images of the inside of the joint onto a monitor. Through the other tiny incisions, the surgeon uses specialized miniature instruments, such as a shaver or radiofrequency device, to carefully remove the inflamed synovial lining while preserving the healthy parts of the joint.
Q5. What type of anesthesia is used for this procedure?
An arthroscopic synovectomy is typically performed using a combination of general anesthesia and a regional nerve block:
- General Anesthesia: This puts you to sleep during the surgery so you feel no pain.
- Regional Nerve Block: An injection is given near the nerves in your neck or shoulder before surgery. This numbs the entire arm, providing excellent pain relief for 12 to 24 hours after the procedure.
Q6. How should I prepare for my surgery?
To prepare for your surgery, you should:
- Follow fasting instructions (no food or drink after midnight before the procedure).
- Discuss all current medications with your doctor, as you may need to stop blood thinners, certain vitamins, or anti-inflammatory drugs a few days before surgery.
- Arrange for a responsible adult to drive you home and stay with you for the first 24 hours.
- Prepare comfortable, loose-fitting clothing that is easy to put on over a bulky bandage or sling (like a button-up shirt).
Q7. What can I expect on the day of surgery?
On the day of surgery, you will arrive at the surgical center or hospital, change into a gown, and meet with your surgical team and anesthesiologist. The nerve block will be administered, and you will be taken to the operating room. The surgery itself usually takes between 45 and 90 minutes, depending on the amount of tissue to be removed. Afterward, you will wake up in the recovery room with a bandage on your shoulder and your arm resting in a sling.
Q8. Will I need to wear a sling after surgery, and for how long?
Yes, you will wear a sling immediately after surgery. However, because a synovectomy does not typically involve repairing torn tendons or ligaments, the sling is mostly used for comfort and protection while your arm is numb from the nerve block. You may only need to wear it for a few days to a week. Your surgeon will give you specific instructions, which may vary if other procedures (like a tendon repair) were performed at the same time.
Q9. How is pain managed immediately after surgery?
Managing pain is a top priority, and your team will use a multi-faceted approach:
- Nerve Block: Provides complete numbness for the first day.
- Oral Medications: Your doctor will prescribe pain relievers (like anti-inflammatories or mild narcotics) to take before the nerve block wears off.
- Ice Therapy: Applying ice or using a cold therapy unit for 20 minutes at a time helps reduce swelling and ease pain.
- Elevation: Keeping your upper body slightly elevated helps minimize throbbing.
Q10. What is the typical recovery timeline?
Recovery timelines vary, but most patients follow a general progression:
- Weeks 1–2: Pain and swelling gradually decrease; light daily activities are permitted; physical therapy begins.
- Weeks 3–6: Range of motion improves; you can perform light exercises and return to light office work.
- Months 2–3: Shoulder strength increases; you can participate in most daily tasks and moderate physical activities.
- Months 3–6: Full recovery is typically reached, allowing a return to heavy lifting and sports.
Q11. How and when will physical therapy start?
For a synovectomy, starting movement early is critical to prevent the joint from becoming stiff and forming scar tissue (adhesions). Physical therapy usually starts within the first week after surgery. Initially, exercises will focus on gentle, passive range of motion (where a therapist or your other arm moves the joint). Gradually, you will progress to active movements and strengthening exercises as the shoulder heals.
Q12. What is the best way to sleep after a shoulder synovectomy?
Sleeping can be challenging during the first few weeks. The most comfortable position is usually in a semi-reclined position (at a 45-degree angle), such as in a recliner chair or propped up with pillows in bed. Placing a small pillow under your elbow or behind your shoulder on the surgical side helps support the arm and prevents it from rolling backward, which can cause pain.
Q13. When can I return to work, driving, and daily activities?
Your return to activities depends on your healing and the type of work you do:
- Desk Jobs: Many patients can return to light desk work within 1 to 2 weeks.
- Physical Jobs: Jobs involving heavy lifting or overhead work may require 2 to 3 months of recovery.
- Driving: You should not drive while taking prescription pain medications or while your arm is in a sling. Most patients can drive safely in 1 to 2 weeks, once they have adequate control of the arm.
Q14. What are the potential risks and complications of the procedure?
While arthroscopic synovectomy is generally very safe, any surgery carries some risks. Potential complications include:
- Joint Stiffness: The most common risk, which is managed with early physical therapy.
- Infection: A rare risk that is minimized with sterile techniques and preventative antibiotics.
- Nerve Injury: Extremely rare damage to surrounding blood vessels or nerves.
- Recurrence: The synovial lining can grow back and become inflamed again over time, particularly in chronic inflammatory diseases like rheumatoid arthritis.
Q15. What are the long-term outcomes and success rates?
The long-term outcomes are generally excellent, especially for patients with localized inflammatory conditions or those whose rheumatoid arthritis is well-managed with medication. Most patients experience significant pain relief, a reduction in joint swelling, and improved shoulder mobility. While a synovectomy cannot cure underlying systemic inflammatory diseases, it is highly successful at controlling local symptoms and preserving the joint for many years.
We encourage you to write down any specific questions you have and discuss them thoroughly with your surgeon, doctor, or physical therapist. They are your best resource for personalized advice and care.
Disclaimer: This brochure provides general information and is not a substitute for professional medical advice. Always consult your doctor or qualified healthcare provider with any questions you may have regarding your specific medical condition and treatment plan.
Related articles
Browse all articles
Trusted External Resources
Curated educational materials to help you make informed decisions about your orthopaedic bone & joint conditions.

Orthopaedia

Orthogate Patient Education
