
Distal Clavicle Excision (Mumford Procedure)
Get Clear, Concise Answers to Your Top Questions About Distal Clavicle Excision (Mumford Procedure)
Q1. What is a distal clavicle excision, and what is the Mumford procedure?
A distal clavicle excision, also known as the Mumford procedure, is a surgical operation that involves removing a small portion (typically 8 to 10 millimeters) of the outer end of the collarbone (clavicle) where it meets the shoulder blade. This creates extra space in the joint, stopping the bones from rubbing against each other and relieving pain.
Q2. What is the acromioclavicular (AC) joint, and how does it cause shoulder pain?
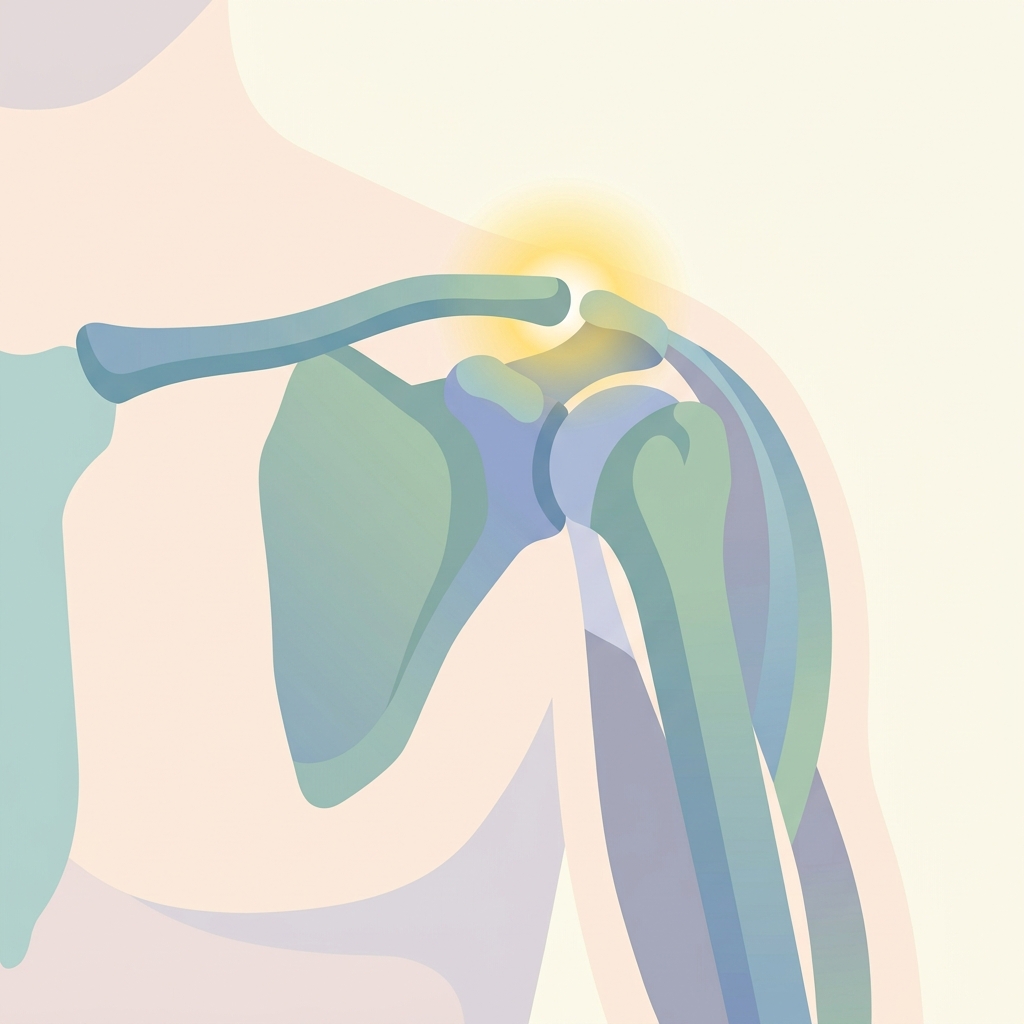
The acromioclavicular (AC) joint is the junction at the top of the shoulder where the collarbone (clavicle) connects to the acromion, which is the bony tip of the shoulder blade. Over time, wear and tear, repetitive overhead use, or injuries can cause the cartilage between these bones to wear down, leading to bone-on-bone friction, inflammation, bone spurs, and significant pain.
Q3. What conditions are treated with a distal clavicle excision?
This procedure is primarily used to treat:
- AC Joint Osteoarthritis: Age-related wear and tear of the joint cartilage.
- Distal Clavicle Osteolysis: Softening or resorption of the end of the collarbone, often caused by repetitive heavy lifting (weightlifter's shoulder).
- Post-Traumatic Arthritis: Damage to the joint resulting from a past separation or fracture.
- Impingement Syndrome: Bone spurs on the AC joint that pinch the underlying rotator cuff tendons.
Q4. How is the Mumford procedure performed?
The surgery is usually performed arthroscopically (using a small camera and tiny instruments inserted through small incisions). During the procedure, the surgeon inspects the shoulder joint, cleans out damaged tissue, and uses a specialized burr to shave away the worn-out end of the collarbone. In some cases, it may be performed through a small open incision if other procedures are being done at the same time.
Q5. What are the benefits of the arthroscopic approach compared to open surgery?
The arthroscopic approach offers several advantages:
- Smaller incisions and less scarring.
- Less damage to the surrounding muscles and ligaments.
- Reduced pain after the operation.
- A faster recovery and rehabilitation process.
Q6. What type of anesthesia is used for this surgery?
Most patients receive a combination of general anesthesia (which puts you to sleep) and a regional nerve block. The nerve block numbs the nerves in your shoulder and arm, providing excellent pain relief for 12 to 24 hours after the procedure, which helps reduce the need for strong pain medications immediately after surgery.
Q7. How long does the surgery take, and will I need to stay in the hospital?
The surgery itself usually takes about 30 to 45 minutes. It is performed as an outpatient procedure, meaning most patients can go home the same day, once the anesthesia wears off and it is safe to travel.
Q8. What are the potential risks and complications of a distal clavicle excision?
While the Mumford procedure is very safe, any surgery carries some risks. These include:
- Infection or bleeding.
- Numbness around the incision site.
- Continued shoulder pain or stiffness.
- Incomplete bone removal, which may require revision.
- Minor instability of the AC joint if too much bone is removed.
Q9. How is pain managed immediately after surgery?
Pain is managed using a combination of methods:
- Nerve Block: Numbs the shoulder for the first day.
- Oral Medications: Prescribed pain relievers and anti-inflammatory drugs.
- Ice Therapy: Applying ice packs for 20 minutes at a time to reduce swelling.
- Rest: Limiting arm movement and keeping the shoulder supported.
Q10. How long will I need to wear a sling after the procedure?
You will typically wear a sling for comfort and protection for about 1 to 2 weeks. Unlike rotator cuff repair, the bone removal itself does not require long-term immobilization to heal. You can usually remove the sling for light daily activities, showering, and structured exercises as directed by your surgeon.
Q11. How should I sleep after the surgery?
Sleeping can be challenging in the first few weeks. To sleep more comfortably:
- Sleep in a semi-upright position in a recliner chair or propped up with pillows in bed.
- Place a pillow behind your elbow or under your arm to prevent your shoulder from falling backward.
- Avoid sleeping directly on your stomach or on the side that was operated on.
Q12. When can I return to normal daily activities like driving and showering?
Most patients can return to light daily tasks within a few days to a week. You can shower once your incisions are dry and closed, typically 3 to 5 days after surgery, keeping the incisions covered. You should not drive while taking prescription pain medications or while your arm movement is significantly restricted.
Q13. When does physical therapy start, and what does it involve?
Physical therapy typically begins within the first 1 to 2 weeks after surgery. The rehabilitation program includes:
- Phase 1 (Weeks 1-2): Gentle passive range-of-motion exercises to prevent stiffness.
- Phase 2 (Weeks 2-6): Active movements to restore full shoulder mobility.
- Phase 3 (Weeks 6+): Progressive strengthening exercises for the shoulder and surrounding muscles.
Q14. What is the recovery timeline for returning to work and sports?
The timeline depends on your activity level:
- Desk Jobs: 1 to 2 weeks.
- Light Lifting/Light Manual Work: 4 to 6 weeks.
- Heavy Manual Labor & Weightlifting: 3 to 4 months.
- Overhead Sports (Tennis, Swimming): 3 to 4 months.
Q15. What are the long-term results and success rates of the Mumford procedure?
The long-term success rate of the Mumford procedure is very high, with over 85% to 90% of patients experiencing significant pain relief and improved shoulder function. Once the bone-on-bone rubbing is eliminated and the joint heals, most patients can return to their previous activities without chronic pain.
We encourage you to write down any specific questions you have and discuss them thoroughly with your surgeon, doctor, or physical therapist. They are your best resource for personalized advice and care.
Disclaimer: This brochure provides general information and is not a substitute for professional medical advice. Always consult your doctor or qualified healthcare provider with any questions you may have regarding your specific medical condition and treatment plan.
Related articles
Browse all articles
Trusted External Resources
Curated educational materials to help you make informed decisions about your orthopaedic bone & joint conditions.

Orthopaedia

Orthogate Patient Education
